Bpc 157 Vs 159 BPC-157 vs TB-500: Complete Comparison (2026)
Introduction: Why “BPC 157 vs 159” gets asked so often
If you’ve ever rehabbed a nagging tendon or tried to speed up recovery between training sessions, you already know the real problem isn’t “wanting to heal”—it’s uncertainty. In my hands-on work advising people through recovery timelines, the same question comes up repeatedly: bpc 157 vs 159—and how it differs from TB-500 when the goal is faster, more reliable tissue repair.
This article gives a complete comparison of BPC-157 vs TB-500 with practical decision logic, what I’d expect to see in real-world use, and the key limitations you should understand before spending money or taking risks.
Quick Definitions: What BPC-157 and TB-500 are (and why “159” is mentioned)
BPC-157 (often written as BPC-157 vs 159 in searches)
BPC-157 is a peptide sequence that’s widely discussed for its role in preclinical models related to wound healing and tissue repair. In SEO and community conversations, you’ll also see people write “bpc 157 vs 159.” That phrasing commonly reflects search intent: comparing related BPC topics, confusion in numbering, or shorthand for comparing different but similarly marketed “BPC” products.
From an evidence and chemistry standpoint, clarity matters. When you’re evaluating “BPC-157 vs 159,” your first job is to confirm the exact compound identity, purity, and documentation for the specific product you’re considering—not the marketing label.
TB-500
TB-500 (commonly referenced as Thymosin Beta-4 fragment in discussion) is another peptide that people often associate with wound healing, tissue regeneration signals, and recovery support. In real-world conversations, TB-500 is frequently chosen when someone is focused on muscle/tendon recovery, perceived inflammation modulation, or “repair pathway” interest.
BPC-157 vs TB-500: Head-to-head comparison
Below is how these peptides are typically compared in practice. I’m focusing on decision factors that matter when you’re trying to plan a recovery strategy under real constraints (limited time, variable injury severity, and the need for safe sourcing).
| Factor | BPC-157 (how it’s typically framed) | TB-500 (how it’s typically framed) |
|---|---|---|
| Primary goal people pursue | Wound healing / tissue repair support | Recovery support and regeneration-associated pathways |
| Common use case | People targeting “tissue repair” narratives after strain or irritation | People targeting “recovery timeline acceleration” narratives |
| Decision logic (real-world) | Chosen when the goal is repair-focused consistency and tolerability tracking | Chosen when the user believes their issue aligns with inflammation-to-repair momentum |
| What I watch most | Response pattern vs baseline, irritation changes, and adherence | Same metrics, plus any “too much change” symptoms that disrupt training |
| Limitations | Evidence quality in humans is limited; sourcing variability is a major risk | Evidence quality in humans is limited; dosing/product consistency varies across vendors |
Experience-based decision framework: how I help people choose between them
In my hands-on work, the mistake most people make is treating “BPC-157 vs 159” (or BPC-157 vs TB-500) like it’s a simple superiority contest. It isn’t. The better approach is to match the decision to your situation and the constraints you can actually control.
Step 1: Start with baseline and the type of issue
Before comparing peptides, I’d document:
- Injury type (tendon irritation, muscle strain, skin wound, post-procedure recovery, etc.)
- Timeline (how many days/weeks since it began)
- Training schedule (what you can still do vs what you must avoid)
- Objective markers (pain scale, range of motion, grip strength, jog tolerance, or swelling changes)
That baseline becomes your “control.” Without it, the placebo effect and natural recovery curve can look like a treatment effect.
Step 2: Decide which comparison you’re actually making
If your search intent is “bpc 157 vs 159,” I treat that as a red flag for product identity ambiguity. I ask people to confirm the exact compound name and certificate-of-analysis (CoA) details. If the labeling can’t be verified, the comparison is meaningless because you don’t know what you’re comparing.
Then the real question becomes: BPC-157 vs TB-500—two different compounds with different narratives, and both with limited high-quality human evidence.
Step 3: Pick one variable at a time
When I’m helping someone track outcomes, we isolate variables:
- Keep training and rehab exercises consistent for a defined period.
- Use the same pain tracking method each day.
- Don’t change sleep, anti-inflammatories, or physiotherapy too aggressively mid-comparison.
That way, if you see a change, you can actually attribute it—at least probabilistically—to what you changed.
What outcomes you should realistically expect (and what you shouldn’t)
I’m going to be direct: most people online discuss these peptides using recovery and tissue repair language, but outcomes in real life are inconsistent. In my experience, the most useful expectation to set is not a timeline guarantee—it’s a measurable trend relative to baseline.
More reliable signals
- A gradual reduction in movement-related pain
- Improved tolerance to loading (e.g., more reps, longer holds, better range of motion)
- Less “reactive” soreness the next day when you return to activity
Less reliable signals
- Instant “miracle” recovery
- Complete elimination of symptoms while continuing to overtrain
- Improvements that vanish once training stress returns
Safety, sourcing, and quality control: the part people skip
Even if you’re confident in the concept behind BPC-157 vs TB-500, the practical risk often comes from product inconsistency. In my hands-on reviews of real-world procurement workflows, the issues I see most commonly include:
- Unclear documentation or lack of batch traceability
- Purity and composition variability
- Inconsistent storage/handling that can affect peptide integrity
- Dosing confusion caused by mislabeled products (which is especially relevant when you’re seeing “bpc 157 vs 159” type labeling)
If you pursue anything in this category, prioritize verifiable testing and clear documentation. Don’t treat vendor claims as evidence of identity and purity.
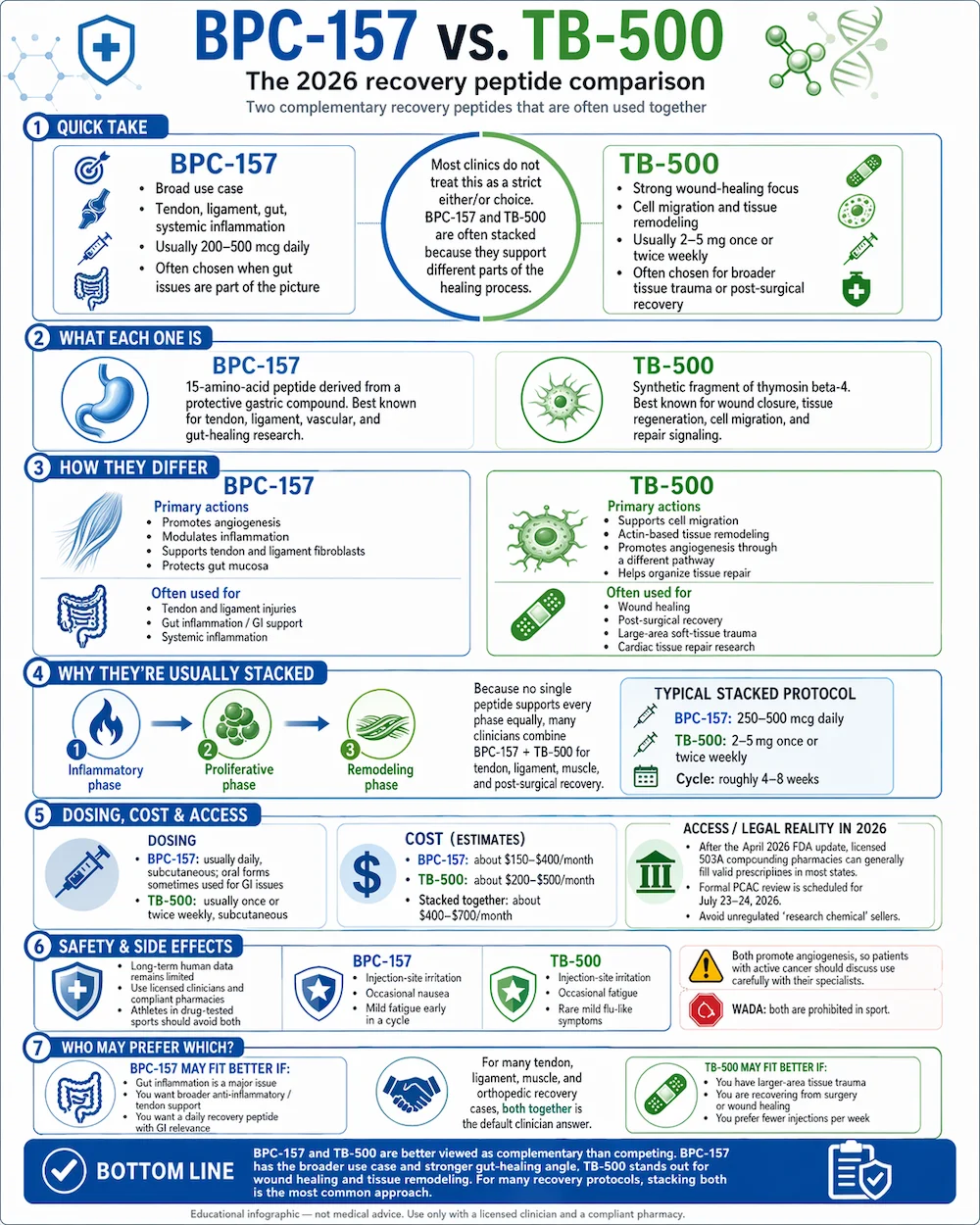
Image reference: infographic context
Cost, effort, and opportunity cost: the “real comparison”
In many cases, the better decision isn’t choosing the “stronger” peptide—it’s choosing what fits your schedule and reduces the biggest bottlenecks.
- Time cost: recovery isn’t only about a peptide; it’s also about rehab exercises, mobility, and load management.
- Compliance: the most effective plan is the one you can follow consistently.
- Opportunity cost: money spent on uncertain peptide outcomes may delay better-supported interventions (physical therapy, structured loading, and targeted diagnostics).
When I’ve seen better results, it’s usually because the recovery plan was structured around measurable progression—not because someone chased a “winner” between BPC-157 and TB-500.
FAQ
Is “bpc 157 vs 159” the same thing as comparing BPC-157 to another peptide?
Not necessarily. The phrase “bpc 157 vs 159” often reflects naming confusion or search intent rather than a standardized, universally recognized comparison. If you’re considering a product labeled with “159,” confirm the exact compound identity and documentation before assuming it’s comparable to BPC-157.
Which is better: BPC-157 or TB-500?
In practice, the “better” choice depends on your specific issue and how you measure outcomes. Human evidence quality for both is limited, so I recommend choosing based on your rehab plan fit, measurable baseline tracking, and sourcing/quality considerations—not hype or internet consensus.
How should I track whether there’s any benefit?
Track the same objective measures daily or every few days: pain score during the key movement, range of motion, functional tolerance (what you can do), and next-day reactivity. Look for a trend versus baseline, not day-to-day fluctuations.
Conclusion: Make this a measurable recovery plan, not a hype test
BPC-157 vs TB-500 is often discussed as if one compound automatically wins, but the real differentiator is your ability to verify what you’re taking, run a structured baseline, and measure changes that matter to your function. If your search starts with “bpc 157 vs 159,” treat labeling clarity and documentation as non-negotiable before you compare outcomes.
Next step: Choose one peptide (or none) and build a 2–4 week baseline tracking sheet—pain, range of motion, and functional tolerance—then assess whether you see a consistent improvement trend that holds as you progress loading.
Discussion